
Report
Observations on Development of Cutaneous Lesions from Bites by the Common Bed Bug, Cimex lectularius L.
Goddard, J., Edwards, K.T., and de Shazo, R.D.
Department of Biochemistry, Molecular Biology, Entomology, and Plant Pathology, Mississippi State University; Department of Medicine, University of Mississippi Medical Center
Received: 7-VI-2011 Accepted: 16-VI-2011
Introduction
Bed bug infestations continue to increase in number, scope, and geographic distribution (Potter 2006, Reinhardt and Siva-Jothy 2007, Romero et al. 2007, Potter et al. 2010). Bed bug bites should be included in the differential diagnosis of common forms of papulosquamous dermatitis including those resulting from other arthropod bites (Goddard and de Shazo 2008). A variety of clinical reactions to bed bugs have been reported most of which have been attributed to immunologic reactions to bed bug saliva, body proteins, or feces (Goddard and de Shazo 2009). Both cell-mediated (Hamburger and Dietrich 1937, Sansom et al. 1992) and IgE-mediated immunologic mechanisms have been proposed (Parsons 1955, Leverkus et al. 2006).
It is possible to gain information about the pathogenesis of cutaneous reactions by determining the timing of the reactions, i.e., immediate, late, delayed, or biphasic (de Shazo et al. 1984). The purpose of this study was to observe macroscopically the evolution of cutaneous bed bug bite reactions in a volunteer who had never knowingly been bitten by bed bugs but who subsequently developed persistent cutaneous reactions to their bites.
Materials and Methods
A post-doctoral researcher (KTE), who had never knowingly been bitten by bed bugs, placed 4 adult bed bugs on the dorsal aspect of her right arm, approximately 28 cm distal to her elbow (Fig. 1). The exact feeding site was noted. Bugs were allowed to feed to repletion (approx. 10 min), then placed in plastic vials for oviposition. Careful observations were made daily as to the development of cutaneous reactions at the bite sites. Seven days after the first biting event, 4 more adult bed bugs were placed on her other arm (left) in the same location. Only 3 of these bed bugs fed to repletion. Again, careful observations were made, and both arms were examined daily for the next 3 weeks. The intensity of the reactions (pruritis, erythema, induration) were rated by the researcher on a Lichert scale (1–10) (Fig. 2).
Results and Discussion
No itching, pain, or cutaneous reactions occurred on the right arm until 5 days after exposure, when bright red, pruritic macules appeared at all bite sites. Itching became increasingly intense over the next 24

Figure 1. Right arm, bed bugs placed for feeding.
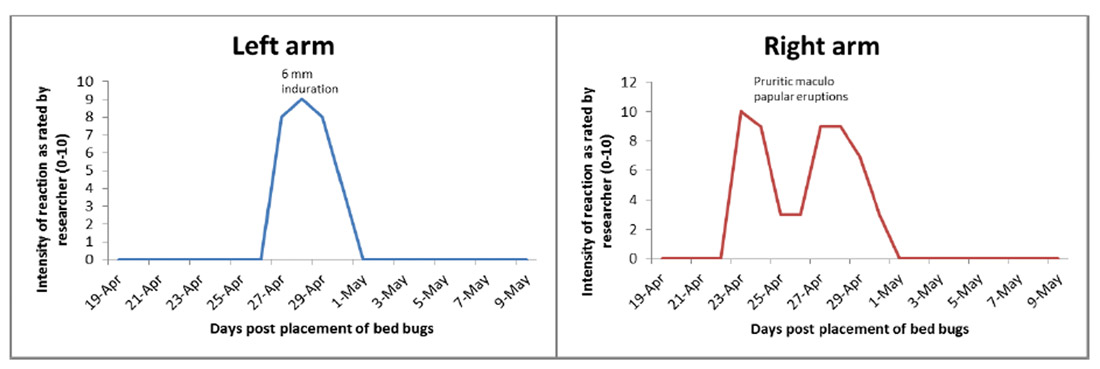
Figure 2. Lesion development curves.
hours, a topical antipruritic cream was applied and oral antihistamines were taken. By day 7, the maculo-papular lesions were still clearly visible, but itching had subsided.
During the second feeding on the left (other) arm, the researcher developed pruritis at the site of previous bites on her right arm. Two days later, induration occurred and was manifested by edema and erythema that developed at the feeding sites on the left arm, peaking in diameter (6 cm) approximately 12 hours later (Fig. 3). This induration subsided, followed by development of pruritic, erythematous maculopapular lesions by day 4 (Fig. 4). Surprisingly, when induration developed on her left arm, the sites of previous bites on her right arm became erythematous and pruritic again (Fig. 5). Bite lesions on both arms resolved over the next 10 days, but faint erythemata at bite sites remained visible (Figs. 6–7). There was some evidence of hyperpigmentation on both arms at the bite sites 21 days post-bite (Fig. 8).
Cutaneous reactions with immunologic mechanisms have been described clinically by the timing of their appearances as “immediate” (within 30 minutes), “late” (6–8 hours), or “delayed” (24–48 hours). Immediate and late reactions have been associated with the presence of a specific antibody to the antigen deposited in the skin while delayed reactions have been associated with cell-mediated mechanisms (Joneja and Bielory 1994). The cutaneous reactions noted here occurred later than did the immediate, late, or biphasic reactions to fire ant venom, insulin, or delayed reactions to purified protein derivative (PPD) and appear similar to the previously reported blistering reactions occurring days after bites (Sansom et al. 1992, Leverkus et al. 2006) and might be unique. Although immediate, IgE-mediated immunologic reactions to insect salivary antigens have been implicated in bullous reactions (Leverkus et

Figure 3. Left arm, induration 3 days post-bite.

Figure 4. Left arm, bite lesions 4-days post-bite.

Figure 5. Right arm, 10 days post-bite.

Figure 6. Right arm, 17 days post-bite.

Figure 7. Both arms, 4 days post-bite (left arm in front), and 11 days post bite (right arm in back).

Figure 8. Right arm, hyperpigmentation 21 days post-bite.
al. 2006), such reactions in our clinical experience have been seen more commonly in reactions to
tuberculin proteins in hyper-immunized individuals. The “lighting-up” phenomenon at sites of previous lesions seen here has been reported anecdotally previously (McKiel and West 1961), but is poorly understood. This presumably results from antigens residing at the bite site for an extended period of time, and from these antigens responding to inflammatory mediators circulating to new bites. Hopefully, the observations reported here will add to the body of information necessary to guide further research to elucidate bed bug bite reactions and their underlying pathology.
References
de Shazo, R. D., C. Griffing, T. Kwan, W. A. Banks, and H. F. Dvorak. 1984. Dermal hypersensitivity reactions to imported fire ants. J. Allergy Clin. Immunol. 74: 841-847.
Goddard, J., and R. D. de Shazo. 2008. Rapid rise in bed bug populations: the need to include them in the differential diagnosis of mysterious skin rashes. South. Med. J. 101: 854-855.
Goddard, J., and R. D. de Shazo. 2009. Bed bugs (Cimex lectularius) and clinical consequences of their bites. J. Am. Med. Assoc. 301: 1358-1366.
Hamburger, F., and A. Dietrich. 1937. Lichen urticatus exogenes. Acta Paediat. 22: 420.
Joneja, J. V., and L. Bielory. 1994. Understanding Allergy, Sensitivity, and Immunity. Rutgers University Press, New Brunswick, NJ.
Leverkus, M., R. C. Jochim, S. Schad, E. B. Brocker, J. F. Andersen, J. G. Valenzuela, and A. Trautmann. 2006. Bullous allergic hypersensitivity to bed bug bites mediated by IgE against salivary nitrophorin. J. Invest. Dermatol. 126: 91-6.
McKiel, J. A., and A. S. West. 1961. Nature and causation of insect bite reactions. Ped. Clin. N.A. 8: 795-814.
Parsons, D. J. 1955. Bed bug bite anaphylaxis misinterpreted as coronary occlusion. Ohio State Med. J. 51: 669.
Potter, M. F. 2006. The perfect storm: an extension view on bed bugs. Am. Entomol. 52: 102-104.
Potter, M. F., B. Rosenberg, and M. Henriksen. 2010. Bugs without borders: defining the global bed bug resurgence. Pest World, Sept/Oct: 8-20.
Reinhardt, K., and M. T. Siva-Jothy. 2007. Biology of the bed bugs. Ann. Rev. Entomol. 52: 351-374.
Romero, A., M. F. Potter, D. A. Potter, and K. F. Haynes. 2007. Insecticide resistance in the bed bug: a factor in the pest's sudden resurgence? J Med Entomol 44: 175-8.
Sansom, J. E., N. J. Reynolds, and R. D. G. Peachy. 1992. Delayed reaction to bed bug bites. Arch. Dermatol. 128: 272-273.